International Journal of Clinical Case Reports 2018, Vol.8, No.2, 5-9
7
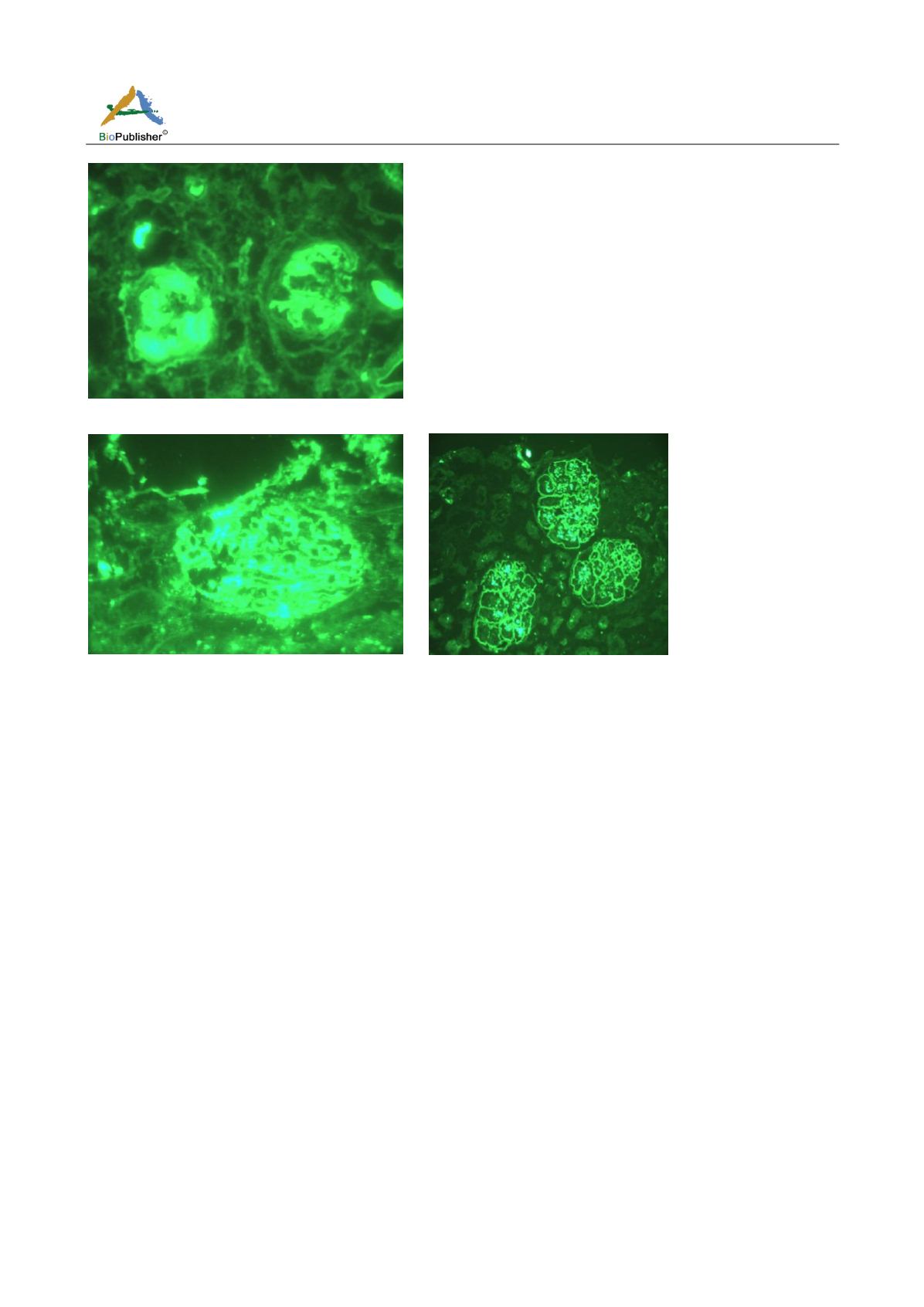
Figure 9 Immunofluorescence showing mesangial deposits of IgG and C3
Figure 10 Immunofluorescence showing granular deposits of IgG
2 Discussion
SLE has a complex etiopathogenesis including genetic factors, drug induced, viral infection, sun exposure and
estrogen. Clinical features of SLE are diverse as it affects joints, lungs, nervous system, kidneys and skin. The
initial complaint starts with fever, malaise, joint pain, muscle pain and fatigue. While SLE is more common in
females than males, the symptoms associated with each sex are different. Females tend to have greater relapses,
decreased WBCs, Raynaud‘s phenomena, arthritis and psychiatric symptoms while males have kidney diseases,
serositis, skin rash and peripheral neuropathy (Long et al., 1998).
Inflammation caused by SLE may affect many parts of the body. Anemia is a common complication along with
problems in bleeding and clotting time and vasculitis. Patients with SLE are more susceptible to inflammation of
the lung. Many people with lupus complain of headache, dizziness, behavioural change and memory problems.
Kidney damage is a common complication and may lead to death. The risk of cardiovascular diseases and heart
attack is more common in SLE patients. Many studies suggested increased risk of cancer in SLE patients. Women
with lupus have increased risk of miscarriage. In the oral cavity, long term use of medication to control lupus can
cause root canal calcification, delayed tooth eruption, dilacerations of root, gingival enlargement with bleeding
and viral infections (Burnham et al., 1963).
The main differential diagnoses are Lichen Planus (L.P) and oral leucoplakia, but distinguishing between oral LE,
LP and leucoplakia can be difficult, both clinically and histologically, even when established histopathological
criteria are used (Bottomley and Goodfield, 1995).
The American College of Rheumatology has published criteria for the classification of patients as having SLE
(Figure 11). If a patient has, at any time in his or her medical history, 4 of the 11 criteria documented, the
diagnosis of SLE can be made with approximately 95% specificity and 85% sensitivity.


