International Journal of Clinical Case Reports 2015, Vol.5, No. 49, 1-5
4
most conventional tumors; more rarely other tumors
arising from the posterior hypothalamus can be found
such as astrocytoma, ependymoma and rarel y
craniopharyngioma. Also a CPP can be secondary to
other causes such as hydrocephalus, malformation
syndromes and after irradiation (Bridges et al., 1994).
The idiopathic forms predominate in girls. They have
no clinical or hormonal characteristics. The evolution
is variable, generally fast as it was noted in patients of
this study (Brauner et al., 1987). Idiopathic character
of the pathology can only be retained after elimination
of the classic causes of CPP systematically sought.
Precocious pseudopuberty is much less common and
refers to conditions in which increased production of
sex steroids is gonadotropin-independent. Correct
diagnosis of the etiology of sexual precocity is critical,
because evaluation and treatment of patients with
precocious pseudopuberty is quite different than that
for patients with central precocious puberty.
Congenital adrenal hyperplasia is a common etiology
of iso-sexual precocious puberty in boys (Bridges et
al., 1994; Agboola-Abu et al., 1999). In our series, it
represents the exclusive cause (Figure 4).
Precocious puberty is observed in case of significant
delay in the diagnosis of the congenital adrenal
hyperplasia and delay in the initiation of substitute
and suppressive therapy with hydrocortisone. It can be
observed in case of treatment inobservance and if
under-dosing patient. The androgen excess upstream
of the enzymatic block is responsible (after
aromatization to an estrogen) of the development of
secondary sexual characters. In some cases a true
central precocious puberty can be constit ute.
The PPP can be secondary to adrenocortical tumor,
ovarian tumor or more rarely a testicular tumor most
often of interstitial tissue or of Leydig cells (Holland
et al., 1987; De Sousa et al., 2008; Bajpai and Menon,
2011).
The McCune Albright syndrome is a rare cause of
PPPs. More common in girls, it’s diagnosed very early
before 4 years. It is based on the presence of skin latte
tasks, a fibrous dysplasia of bone, and sometimes an
autonomous hypersecretion of endocrine glands
particularly thyroid and ovarian ones (Cavanah and
Dons,1993; Haddad and Eugster, 2007).
These characteristics have been objectified in our
patient, clinically the PP was dominated by
metrorrhagia occurred at the age of one year which
was relevant to with a large ovarian cyst. The
initial endocrine exploration had not found other
endocrinopathies, but the checks carried out revealed
the appearance of a pre toxic thyroid nodule requiring
radical treatment.
Treatment of CPP relies on suppression therapy with
GnRH analogues. The study of the different factors
influencing the adult size shows the importance of
advanced bone age for the size and the age in the
beginning of symptoms. It should however be noted
that patients who have non-progressive or slowly
progressive puberty have a good prognosis without
treatment on the size, due to the absence of major
bone age advance (Kaplowitz and Oberfield, 1999).
Aromatase inhibitors indicated in ovarian or testicular
PPP lead a regression of secondary characters but give
partial results on bone maturation. The specific
treatment of organic causes can control endocrine
disorders (Isguven et al., 2003; Kalfa et al., 2005).
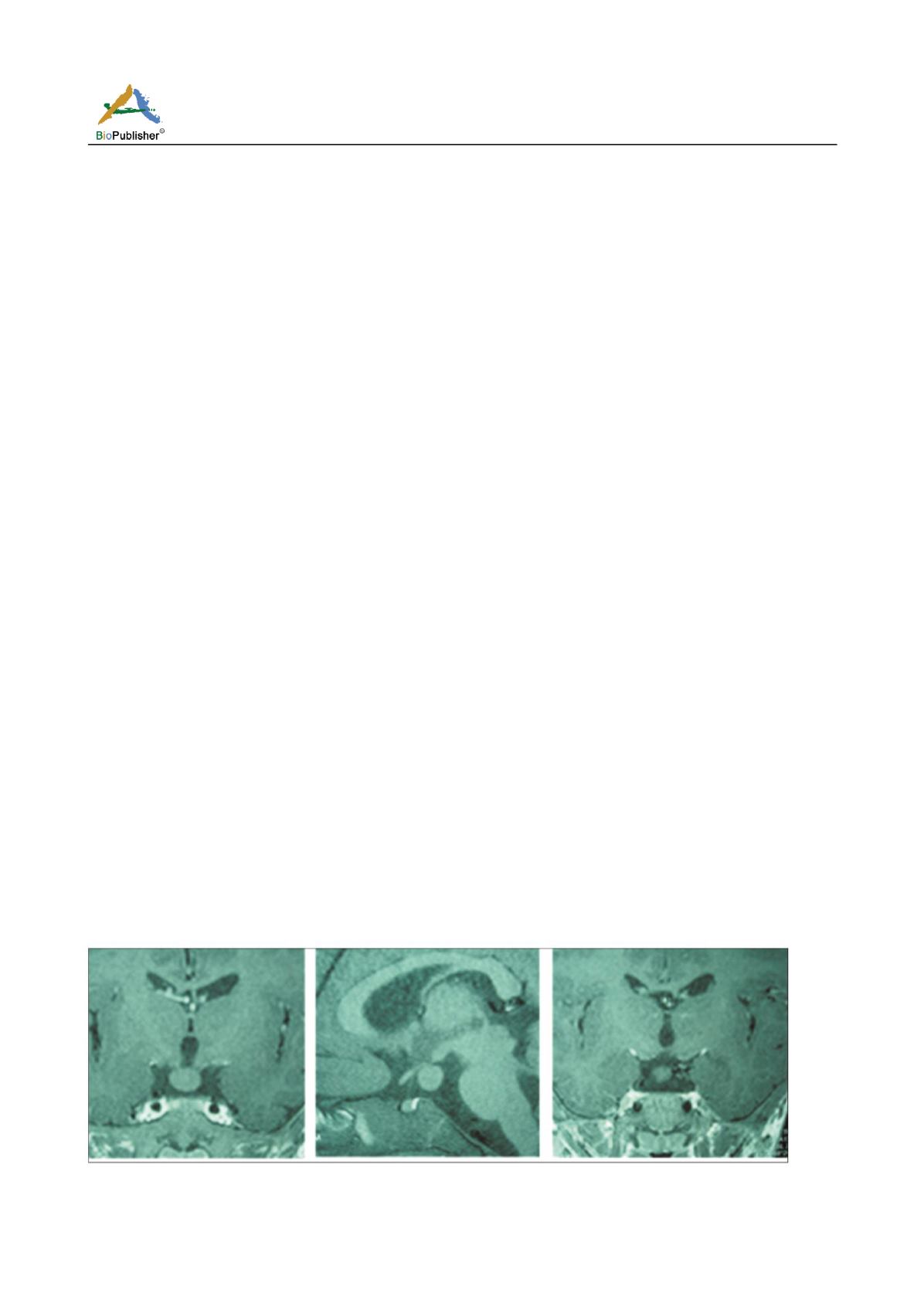
Figure 3 Hypothalamic hamartoma (10 mm) responsible for a scalable central precious puberty in a child of 3 years old


