International Journal of Clinical Case Reports 2015, Vol.5, No. 49, 1-5
3
This condition is met more often in girls than in boys
and occurs at a variable age before 08 years, usually
before 06 years (Mogensen et al., 2011) which has
been objectified in our study. It is important to
distinguish what is only a variant of normal puberty
from true precocious puberty (Parent et al., 2003).
Premature pubarche and premature thelarche are 2
common, benign, normal variant conditions that can
resemble precocious puberty but are non progressive
or very slowly progressive. Premature thelarche refers
to the isolated appearance of breast development,
usually in girls younger than 3 years; premature
pubarche refers to appearance of pubic hair without
other signs of puberty in girls or boys younger than
7-8 years. A thorough history, physical examination,
and growth curve review can help to distinguish these
normal variants from true precocious puberty
(Aksglaede et al., 2009).
The management of the PP is done in three steps:
affirm the reality of pathological puberty, search the
central or peripheral origin also idiopathic or organic
etiology and finally pose an indication of a
suppression therapy of puberty.
The central PP (CPP) is 4-5 times more common
in girls than in boys. The clinical picture is more or
less rich depending on the speed and duration of the
evolution. The combination of breast development in
girls, testes in boys and pubic hair reorients etiological
exploration to a central origin of iso sexual precocity
(Figure 1; 2) (Herman-Giddens et al., 1997). However,
an authentic CPP may present initially as an isolated
development of a secondary sexual characteristic or
even an isolated accelerated of linear growth which
may precede by several months or years the
appearance of secondary sexual characteristics posing
an etiologic diagnosis problem (Brauner et al., 1987).
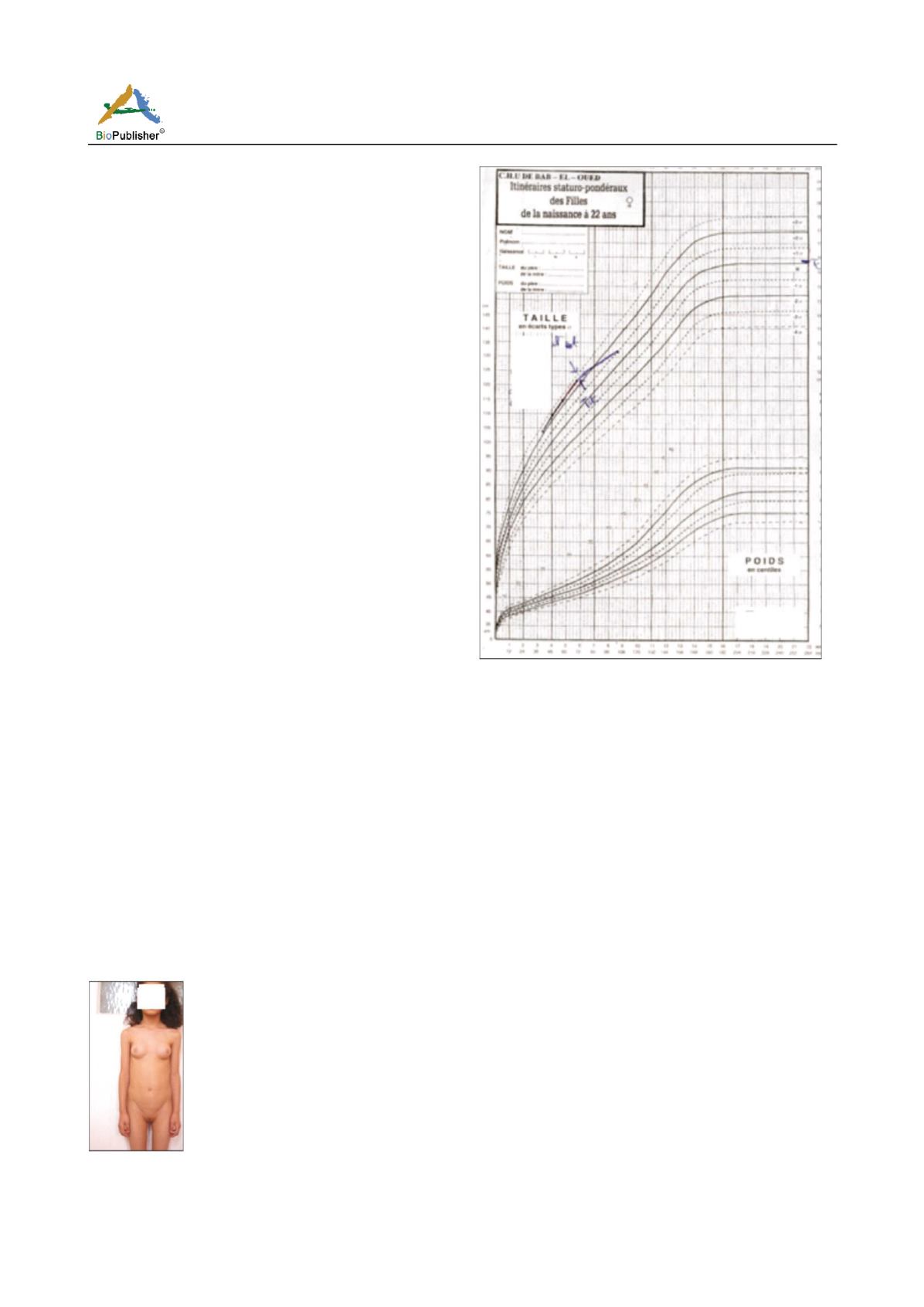
Figure 1 Girl aged 7-year-old t with idiopathic CPP: Breast
development stage S3, pubic hair stage 2 in Tanner, accelerated
growth rate (statural Age 12 years, bone age 11 years)
Figure 2 Deceleration in growth rate suppression therapy by
LHRH analogues in a little girl with PPC
When the diagnosis of PP is affirmed, the study of
plasma gonadotropins can guide the etiologic
diagnosis to a central cause and appreciate the
scalability of puberty while studying the hormonal
response after stimulation with GnRH analogues
(Boepple et al., 1992). The progressive forms are
predominant both in girls and in boys and account for
60-70% of cases (Kaplowitz, 2004). In our study, they
were present at all the boys (100%) and in half of girls
(52.5%).
The organic forms are more frequent than other
etiologies. In boys, they represent 65% of etiologies
(VS 78% in our study). In girls, they are found in 30%
of cases VS 17% in our series (Bridges et al., 1994).
The frequency of intracranial tumors responsible for
CPP is variable and it’s between 7 and 12% in girls
(Ng et al., 2003); and are responsible for 50-80% of
boys CPP (Styne, 1991). In our patients, they were
present in half of the cases represented by
hypothalamic hamartoma (Figure 3). Indeed, the optic
chiasm glioma and hypothalamic hamartoma are the


