International Journal of Clinical Case Reports 2015, Vol.5, No. 42, 1-6
4
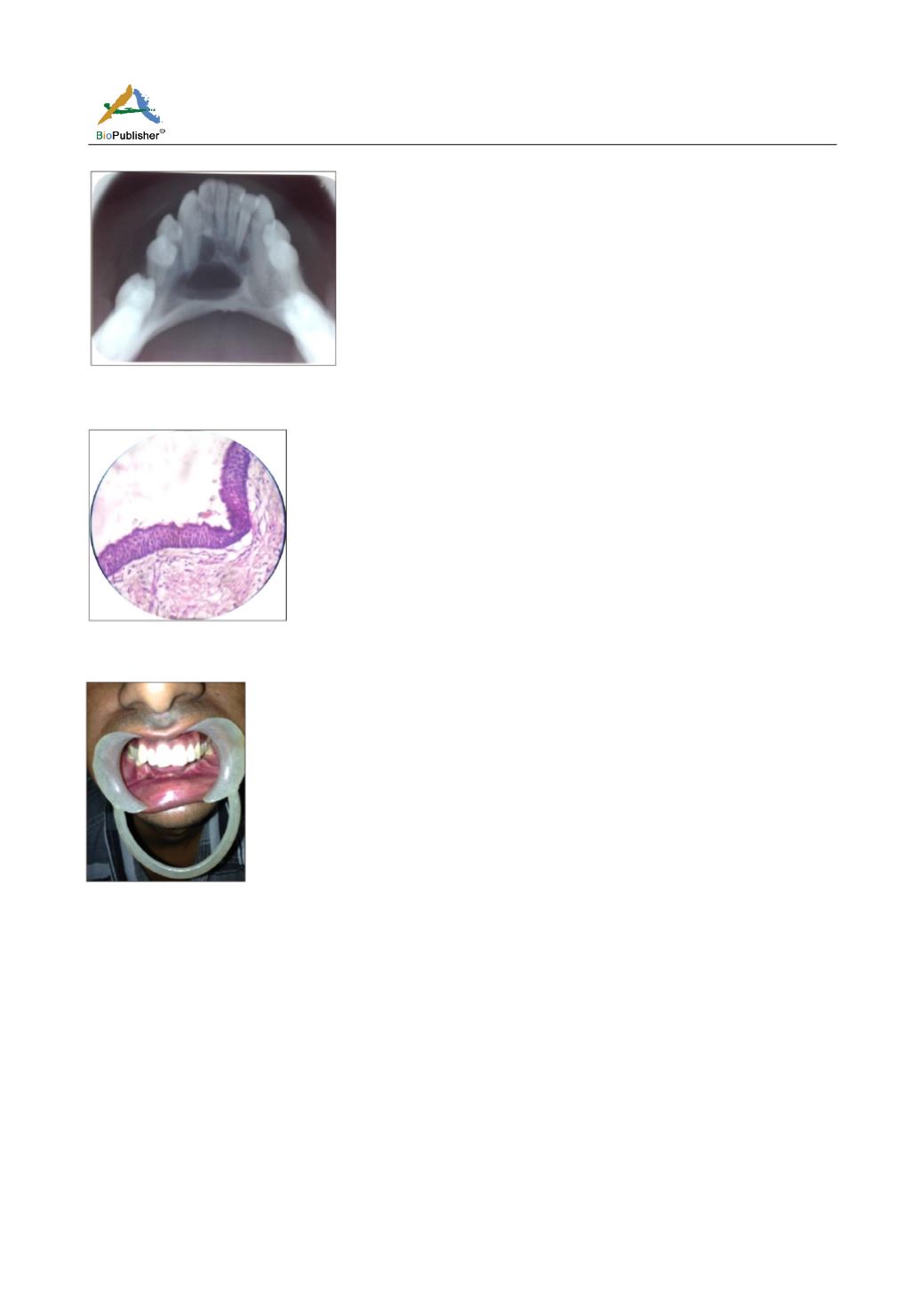
Figure 9
Figure 10
Figure 11
have suggested that OKC should be considered as a
benign tumour and hence be called as KCOT or
keratocystic odontogenic tumour. Shear has countered
this argument by saying that even if it is a neoplasm, it
is suitable to be called as OKC as many neoplasms do
not essentially have a suffix ‘oma’. This debate was
started by Shear (2003) that OKC should be called as
keratocystoma which led Philipsen and Riechert
suggesting keratinising cystic odontogenic tumour in
2004 and then Philipsen suggesting keratocystic
odontogenic tumor again in 2005 (Jyothi et al., 2010).
This cyst has a propensity for recurrence and the
aggressive behaviour clinically and histologically has
necessitated the reclassification of the lesion by the
World Health Organization (WHO, 2005) as a
‘keratocystic odontogenic tumor’ (KCOT). The KCOT
is defined as ‘a benign uni- or multicystic, intra-osseous
tumor of odontogenic origin, with a characteristic
lining of parakeratinized stratified squamous
epithelium and potential for aggressive, infiltrative
behaviour (Çakur et al., 2008; MacDonald- Jankowski,
2011; Rajkumar et al., 2011). Odontogenic Keratocyst
(OKCs) of the jaw is a type of developmental cyst and
there is general agreement that the odontogenic keratocyst
arises from cell rests of the dental lamina. This cyst
shows a different growth mechanism and biologic
behaviour from the more common dentigerous cyst and
radicular cyst (Neville et al., 2002; Avinash et al.,
2010). Around 60% of all cases are diagnosed
odontogenic keratocysts in people typically being
found in adults in the second to fourth decades of life
and with a slight male predilection (M:F=1.6:1). The
age distribution appears to be bimodal. There appears
to be two peaks of incidences between 25-34 years
and 55-65 years of age.The mandible is occupied in
60% to 80% of cases, with a marked tendency to
involve the posterior body and ascending ramus where
anterior mandible is an uncommon site with the lesion
crossing the midline (Neville et al., 2002; Sulabha et al.,
2013). In maxillary region, there are inconsistencies
regarding the predominant location of OKCs. One
study shows that OKCs are distributed evenly between
the anterior and posterior regions of maxilla; some
show that there are more anterior lesions than
posterior lesions and others concluded that the
posterior region is more predominant site (Hiremath et
al., 2011). Patients with keratocysts may complain of
pain, mobility of teeth in the affected area, swelling,
or discharge. Nasal obstruction, paresthesia, and root
erosion are more rare symptoms. Occasionally
diseased person may experience paresthesia of the
lower lip or teeth. In many instances, patients were
amazingly free of symptoms until the cysts reached a
large size and involved the maxillary sinus and the
entire ascending ramus, including the condylar and
coronoid processes. These patients may be unacquainted
of the lesions until they build up pathologic fractures
or may be incidental finding during examination
(Çakur et al., 2008; Avinash et al., 2010). In our case,
the patient did not spontaneously complain of pain,


