International Journal of Clinical Case Reports 2015, Vol.5, No. 42, 1-6
3
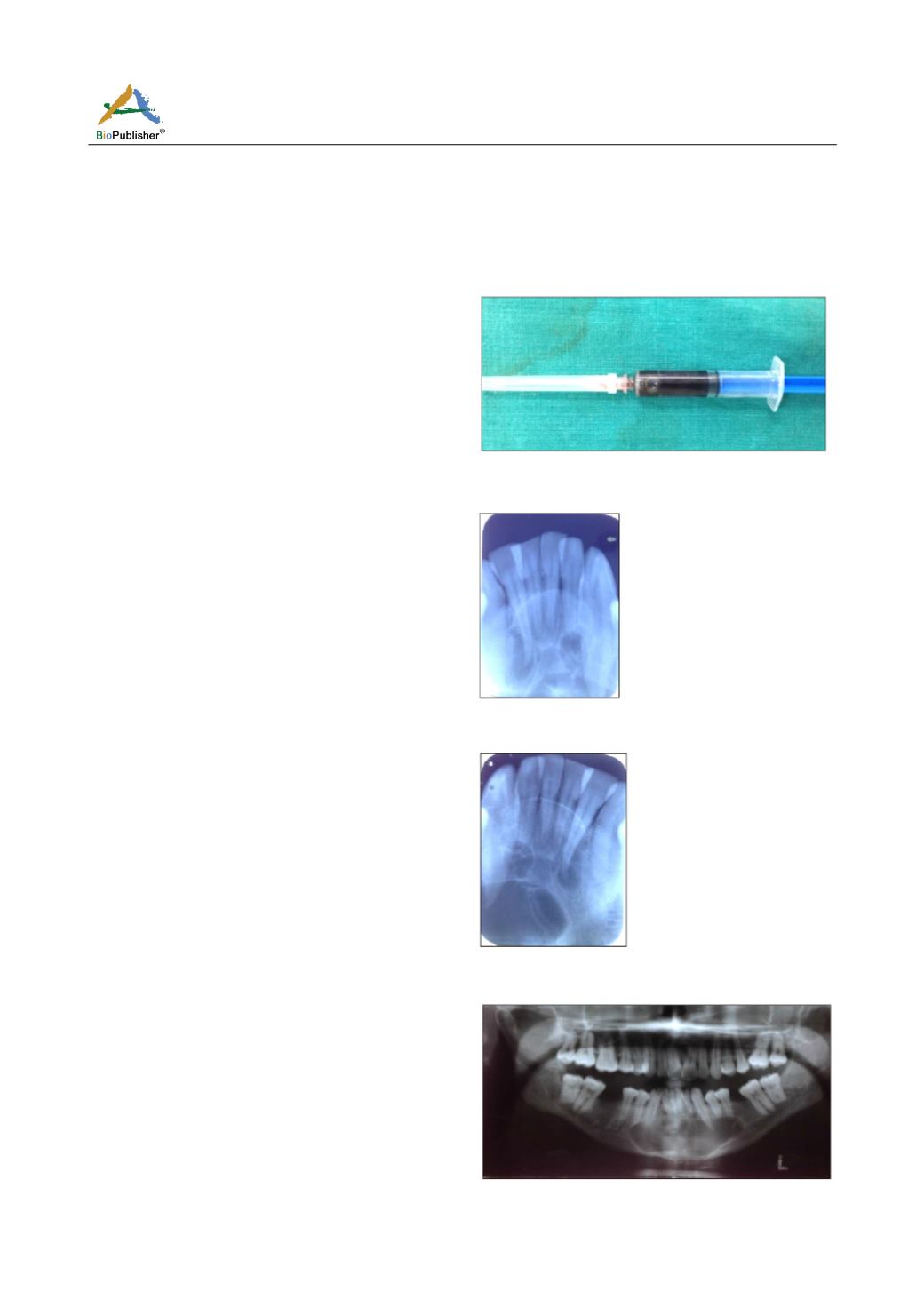
During aspiration, a dark blackish-red betadine coloured
aspirate was taken out (Figure 5). IAOPAR irt 31,
32,33,41,42,43 were advised. IOPAR revealed
multilocular well defined radiolucencies overlapping
each other at the apical regionof 31,32,33,41,42.
Margin of the radiolucencies were sclerotic (Figure 6,
7). Orthopantomogram showed well defined multilocular
radiolucency extending from the periapical region of
35 till the peripical region of 43,44. Sclerotic margin
with displacement of teeth could be appreciated. The
lower border of the radiolucency overlapped and
crossed the inferior border of mandible. Apical 1/3 of
roots in relation to 33,35,43,45 appeared knife edged
suggestive of root resorption (Figure 8). Mandibular
topographic occlusal radiograph was performed to
check the buccolingual expansion. In this radiograph,
multilocular radiolucency was evidently seen in the
apex of 33,32,32,41,42 region. A thin sclerotic line
was also appreciated on the buccal aspect of 32,
33,34,35 suggestive of buccolingual expansion.
Inferior border of mandible appeared intact (Figure 9).
On the basis of clinical examination and chair side
investigations, a provisional diagnosis was made for
central giant cell granuloma with differential diagnosis
of Glandular odontogenic cyst, Aneurysmal bone cyst,
Ameloblastoma, Odontogenic keratocyst, and an
Arteriovenous malformation in relation to 35 to 43
region. The lesion was examined at biopsy. Histopa-
thologically, H & E staining showed epithelia overlying
the connective tissue stroma. The epithelium was
parakeratinized, stratified squamous, 8-10 layer thick.
Basal cells were tall columnar in appearance with
hyperchromatic nuclei, exhibiting reverse polarity.
Loss of cellular adhesion and subepithelial split could
also be seen. Connective tissue stroma showed
juxtaepithelial hyalinization and was sparsely cellular
with loose collagen fibres, acute inflammatory cell
infiltrate and areas of haemorrhage (Figure 10).
Surgical enucleation was performed under all aseptic
precautions and was started antibiotic prophylaxis.
Complete enucleation with aggressive curretage was
performed. Patient was kept under repeated follow-up
for three months. Patient was re-called after 3 months
and after 9 months (Figure 11).
Discussion
An insight into the times past of odontogenic cysts
goes back to the 19th century, when the odontogenic
keratocyst (OKC) was first described in the year 1876
and was named by Phillipsen in 1956 (Neville et al.,
2002) who described it as a different entity characterized
by a keratinized lining, presence of satellite cysts and
association with the nevoid basal cell carcinoma
syndrome (Nagraja et al., 2012). Philipsen and Riechert
Figure 5
Figure 6
Figure 7
Figure 8


