International Journal of Clinical Case Reports 2017, Vol.7, No.7, 28-32
29
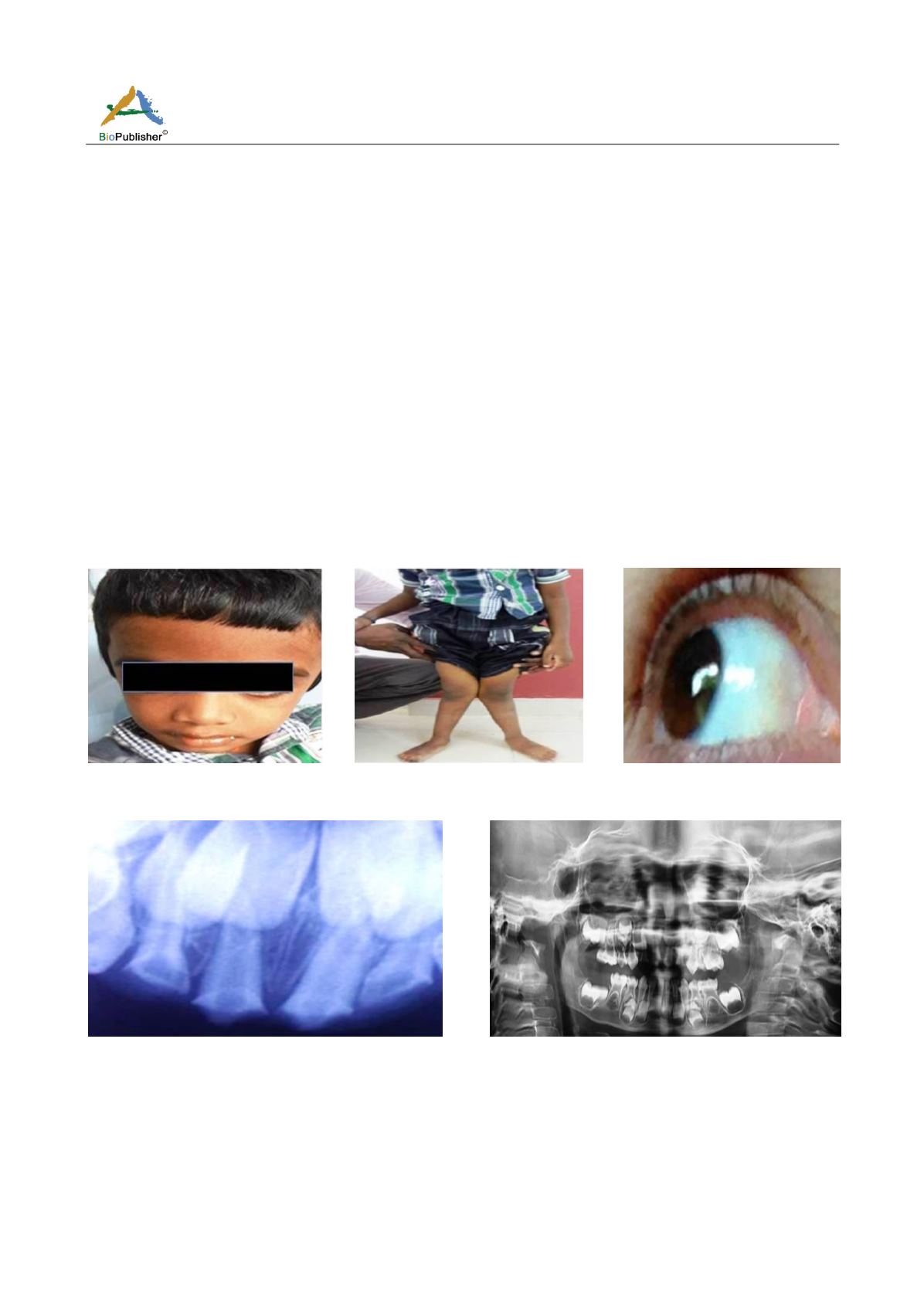
teeth which, however, showed no changes in the periapical region (Figure 4). Orthopantomograph (OPG) of the
patient, also, revealed no significant findings (Figure 5). Although the child presented with a simple diagnosis of
chronic irreversible pulpitis, he was suffering from a major systemic disease. Based on the history of repeated
fractures and presence of bluish tinge in the sclera, a provisional diagnosis of Osteogenesis Imperfecta (OI) was
arrived-at. The patient's parents were advised to get medical reports in the following visit. The child was managed
symptomatically for his dental complaint. The other skeletal diseases which could have presented with childhood
fractures in the differentials included juvenile Paget’s disease, rickets and juvenile osteoporosis for which the
patient's parents were reported to have opinion for to rule-out their possibility and associated adverse effects as for
the preventive strategy (Table 1). In the following visit, the patient presented with medical records confirming
with the diagnosis of Osteogenesis Imperfecta (OI) type 2. His most recent lab investigations were, though, within
normal limits including serum alkaline phosphatase level of 274 IU, a serum calcium level of 8.8 and serum
phosphate level of 5.7. The patient was on oral alendronate once a week along with calcium supplements. Based
on the above, a final diagnosis of chronic irreversible pulpitis (CIP) in Osteogenesis Imperfecta (OI) type 2 was
given. No dental procedure was done considering the patient’s general health condition as per the pediatric
orthopedician’s advice. The parents of the patient were made to realize the need for importance of maintenance of
oral hygiene. A good attempt was made to demonstrate oral hygiene instructions to the child. Osteogenesis
Imperfecta (OI) type 2 is considered to be the most severe type of OI with most of the patients succumbing to
death before or, few year after birth. The patient was kept on regular follow-ups for any needful.
Figure 1 Frontal profile of the patient
Figure 2 Bowed long bones with
knock knees
Figure 3 Bluish tinge in sclera
Figure 4 Intra-oral peri-apical (IOPA) radiograph revealing
no changes in the peri-apical region
Figure 5 Orthopantomograph (OPG) revealing no significant
findings


