International Journal of Clinical Case Reports 2017, Vol.7, No.16, 67-72
70
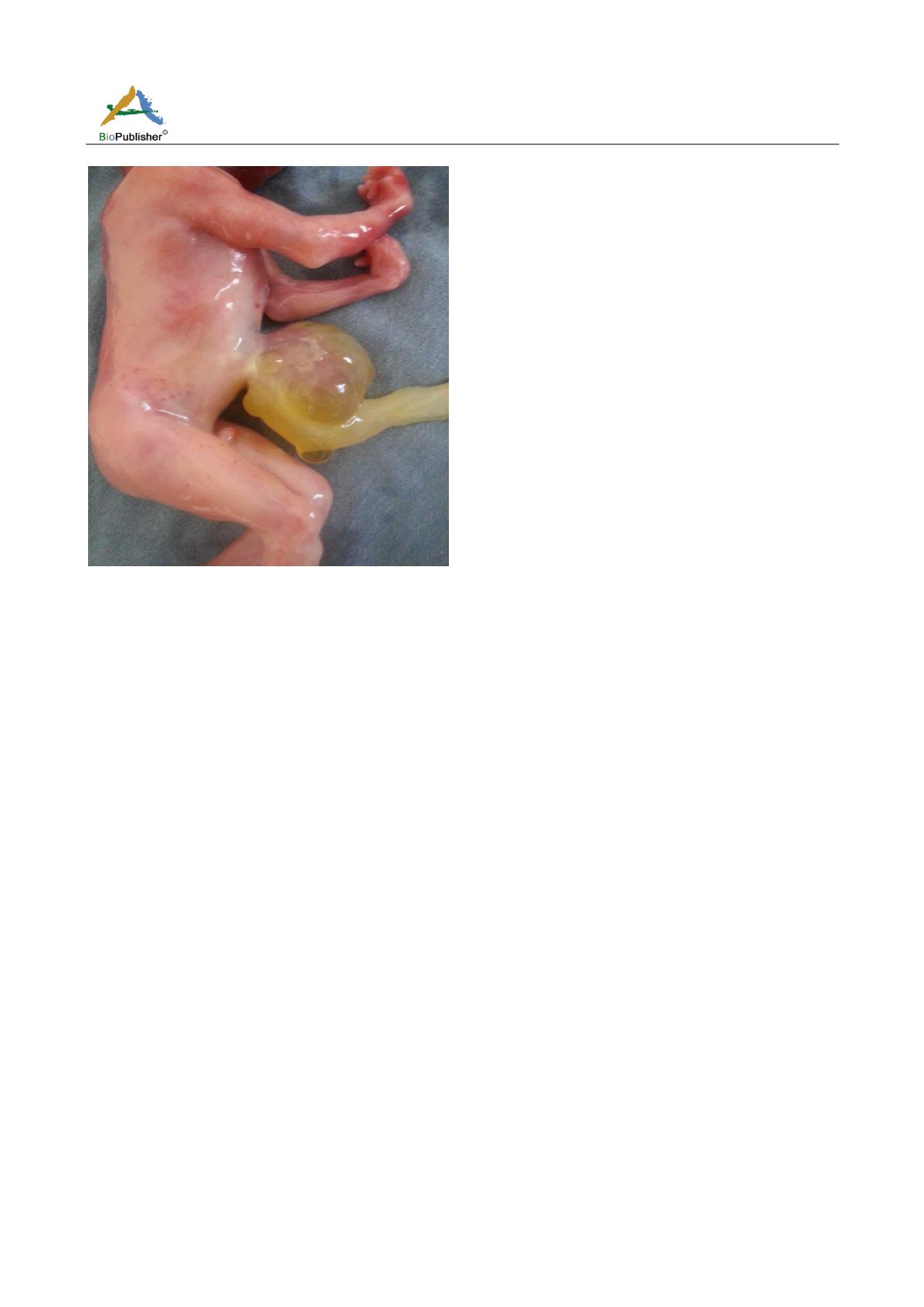
Figure 5
Boy with omphalocele, clenched hands and joint stiffness
2 Discussions
The omphalocele is a central ventral closure defect leading to herniation of the abdominal viscera in the umbilical
cord base. Its frequency varies according to the series of 1/2000 to 1/5000 births (Mohsni et al., 2008). Maternal
age does not appear to be a risk factor (Boog et al., 1993; Fratelli and Parageorghiou, 2007; Weiner and
Goldostein, 2007). Some authors report a higher incidence in male fetuses (Yokoyama and Del Castillo, 2007;
Chen, 2007). In our work, two of our patients were over 38 years old and omphaloceles had interested two boys
and one girl.
The review of the literature identifies several familial cases whether they are omphalocele recurrences in the same
patients (Mohsni et al., 2008) or sporadic familial cases including 8 cases of omphalocele in the same family
(Desselle and Herve, 2007). These familial cases of omphalocele suggest the possibility of a genetic origin
(Fratelli and Parageorghiou, 2007). This risk of recurrence, although low, justifies genetic counseling both in
isolated omphaloceles and associated with a polymalformative syndrome (Chen, 2007). None of our patients had
similar cases in the family.
Thanks to the progress of the ultrasound, the antenatal diagnosis of the omphalocele is made possible in the first
trimester. This diagnosis is usually easy. The omphalocele is in the form of a neoformation appended to the
anterior abdominal wall; its boundaries are clear and distinct from the abdominal contour. Inside this mass existed
heterogeneous echoes, intestinal loops or even hypoechogenic images corresponding to the liver as well as many
other organs that can be highlighted. At the same time, there is a reduction in abdominal circumference. Moreover,
it is easy to find the implantation of the umbilical cord at the level of this neoformation.
Before the 11
th
week, it is difficult to affirm the parietal defect (Yokoyama and Del Castillo, 2007; Tourne and
Chauleur, 2007). However, the presence of echogenic, homogeneous swelling larger than the abdominal diameter
would be in favor of the diagnosis rather than a simple delay in intestinal reintegration into the abdominal cavity
(Boog et al., 1993;
Van Hoorn and Moonen, 2007
). In our case the diagnosis of omphalocele was easy, including
the case revealed in the first trimester of pregnancy.


