International Journal of Clinical Case Reports 2017, Vol.7, No.12, 49-52
50
Obstetric ultrasound showed an evolutionary mono-fetal pregnancy whose biometry is consistent with the term.
Moreover, no morphological abnormality was detected on this examination. The pre-tocolytic assessment revealed
no anomalies. Antenatal corticosteroid therapy based on Celestian and a tocolysis with parenteral Bricanyl had
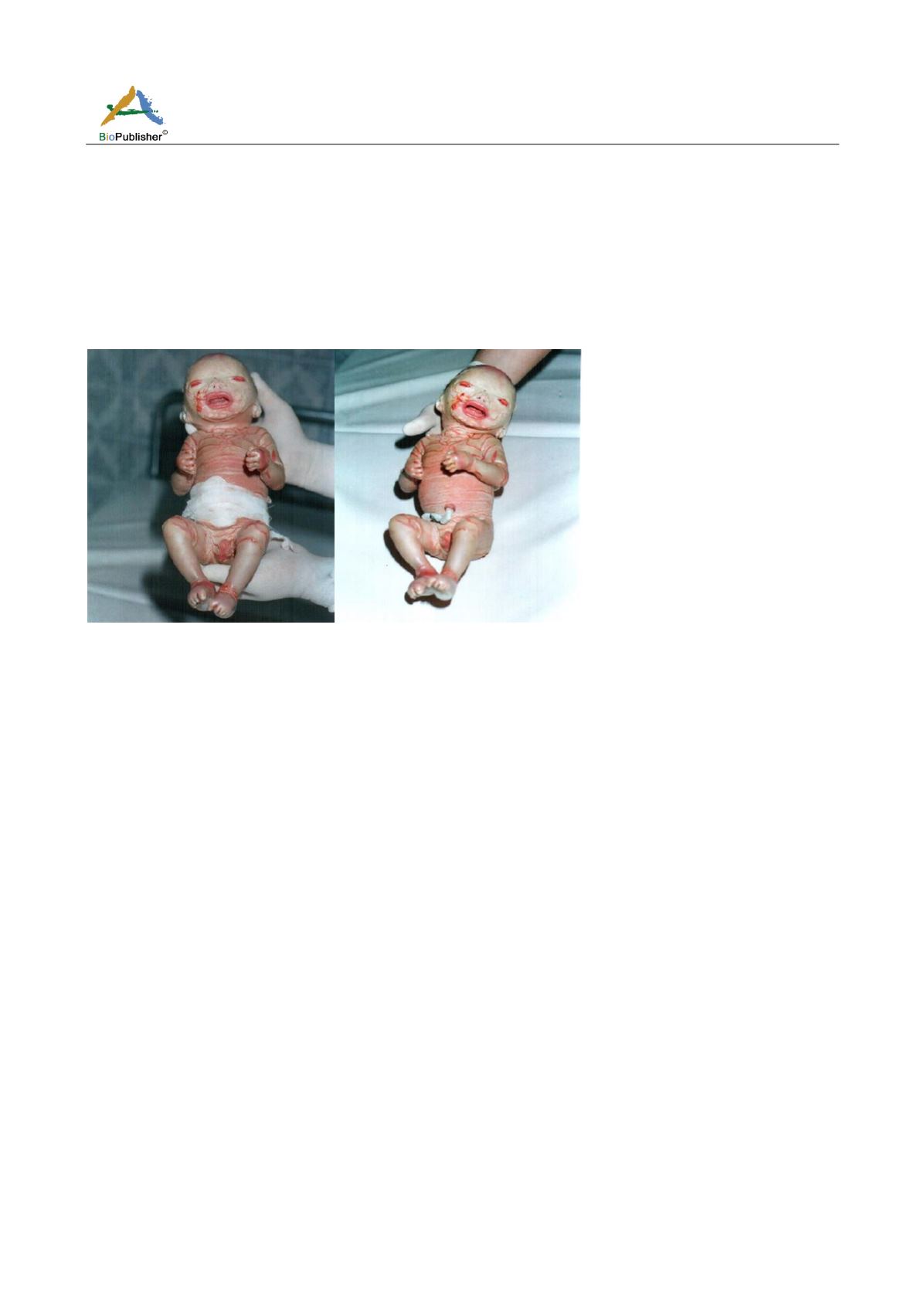
been introduced. The evolution was marked by a premature birth within 24 hours of a male baby, birth weight 1
600 g,
with a taut, glossy skin resembling collodion with an ectropion, an eversion of the lips, wrinkled auricular
flaps and the ends of fingers are slivered
(Figure 1). Its evolution was rapidly fatal within hours. The
fetal-pathological examination had concluded with a collodion fetus. This is a case of recurrent congenital
ichthyosis.
Figure 1
Morphological aspect of a Baby Collodion at birth
2 Discussion
The ichthyosis are described as a heterogeneous group of diseases having as common characteristics the formation
of an abnormal stratum corneum with hyperkeratotic skin lesions which result in generalized desquamation with
or without epidermal hyperproliferation or inflammation of the dermis (Hohl, 2004;
Alam, 2004
)
.
The baby
collodion is the congenital and initial expression of many forms of ichthyosis which it does not allow to prejudge
the severity. The child, at birth, has a skin similar to dry collodion covering the entire epidermal surface.
Exfoliation begins early with cracks in the collodioned membrane. The cracks may remain superficial, or deepen
and touch the superficial dermis (Larrégue et al., 2008). Skin is erythematous, glossy stretched and glazed and
responsible for ectropion,
éclabion
, flattened helix, and flexion of the fingers and toes, the folds are cracked,
sometimes erosive. Semi-mucous membranes, nails and hair are normal. In our observation, the dermatological
lesions were fairly characteristic of the condition, which allowed us to make the diagnosis upon clinical
examination. Moreover, the recurrence of this syndrome within a family until the disease-free, orient us towards a
genetic impairment transmitted in the autosomal recessive mode.
Pathogenesis is not well known. Certain socio-cultural specificities are at the origin of a high rate of consanguinity
and a higher frequency of these hereditary disorders of the keratinization. A minority of collodion babies,
associated with transglutaminase keratinocyte deficiency (TGK) by mutation of transglutaminase 1, are
spontaneously resolving (Mazereeuw
‐
Hautier et al., 2009). Indeed, this benign variant follows an autosomal
recessive transmission and a case caused by a particular mutation with minimal deficiency of keratinocytic
transglutaminase has been reported (Saurat, 2004). The evolution is very variable and unpredictable. Indeed, a
congenital array of collodion baby has been reported in 53% of dry congenital erythroderma and 12% of lamellar
ichthyosis. In 10% of cases, the collodion baby may be the first sign of a common ichthyosis.
In 10% of cases, it is a self-healing baby collodion, whereas in 20% of cases, it can be a Gaucher disease or a
Trichothiodystrophy showing at birth a phenotype of baby Collodion (Larrégue et al., 1986; Ay, 1988; Akiyamam,
1999). The collodion baby is a newborn at high risk. It is often born prematurely (Hohl, 2004), as our case


