基本HTML版本



International Journal of Clinical Case Reports 2014, Vol. 4, No. 6, 1-4
http://ijccr.biopublisher.ca
3
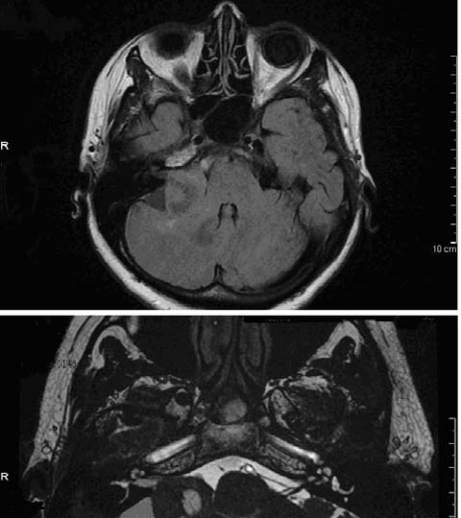
Figure 2 Ovoid lesion of 33
× 23 mm, which presents an inner
cystic-necrotic portion, situated at right cerebellopontine angle.
Another smaller lesion (17 mm) with similar characteristics is
appreciable at left cerebellopontine angle.
Most of VS are solid; cystic VS compose 4%-20% of
all VS and are commonly larger at the time of
presentation (6).
After the imaging, patient was sent to a Neurosurgical
evaluation, preparing the idea of surgery, due to the
size of VS (28 mm), its cystic nature, that did not
recommend gamma knife radiosurgery (1,7), despite
the lack consensus in the literature (8), and
considering her relatively young age (56 years) and
her incoming symptoms (9-10). She was informed on
the three principal possible routes of access to the
surgical removal of VS (translabyrinthine, middle
fossa and retrosigmoid approach) (11,12,13). She was
told that retrosigmoid approach would have been the
preferred, with more likely preservation of facial
nerve’s function, and with minimal risk of persistence
of residual disease (6,14,15). She agreed and she did
not want to delay the possible date of intervention.
VS was macroscopically removed with surgery by
retrosigmoid approach, ten days after diagnosis, with
preservation of seventh cranial nerve (third grade of
House-Brackmann, one week after surgery), but with
ipsilateral hearing loss. After 3 months we saw only a
slight motor deficit (first grade) of the lower branch of
the facial nerve.
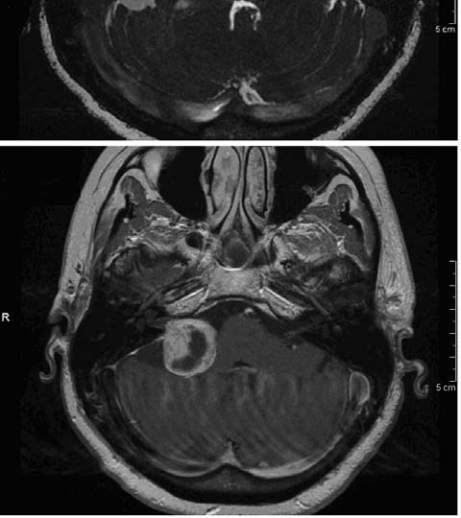
Figure 3-4-5 Cystic VS of 28 mm in the largest extrameatal
diameter, with moderate compression on right middle
cerebellar peduncle and minimal surrounding edema.
Discussion
VS is a rare benign tumor of eight cranial nerve.
Generally its diagnosis is late or occasional. We were