基本HTML版本



International Journal of Clinical Case Reports 2014, Vol. 4, No. 2, 1-5
http://ijccr.biopublisher.ca
3
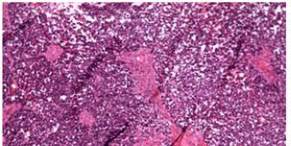
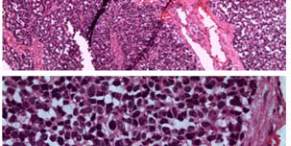
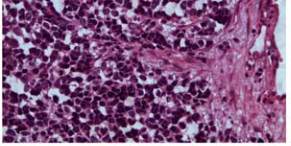
Figure 4 Biopsy was taken and histology showed embryonal
rhabdomyosarcoma
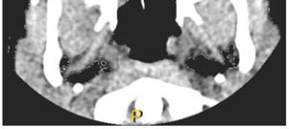
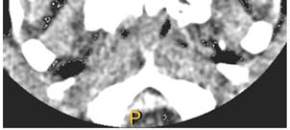
Figure 5 Tumour clear maxillary Sinuses after treatment. Some
residual tumour in the posterior part of the left nasal cavity
Figure 6 Left orbit clear of tumour
2 Discussion
Rhabdomyosarcoma is the most common soft tissue
sarcoma of childhood, representing 5% of all
childhood cancers (Turner, 2011). It arises from
primitive mesenchymal cells committed to skeletal
muscles differentiation and can occur in a variety of
organ and tissues, including those without skeletal
muscles (Turner, 2011). It has an average age of onset
between 4 and 6 years with male preponderance
recorded (Mahour, 1967). Our patient is a 7 years old
boy.
Presenting symptoms vary from patients and is limited
to the site of disease. Pain may be present. If
metastatic disease is present, symptoms of bone pain,
respiratory difficulty (secondary to lung nodules or to
pleural effusion), anemia, thrombocytopenia, and
neutropenia may be present.
Survival of children with rhabdomyosarcoma is
related to the stage and anatomical location of diseases
with bone erosion and malignant cells in cerebral
spinal fluid carrying poor prognosis. It was previously
suggested that histological subtypes were relevantly
unimportant to outcome (Bale, 1986), but recent
evidence shows alveolar subtype responds less
favourably compared to others (Flammant, 1998;
Maurer, 1993).Our patient had embryonal subtype,
and has responded very well to both chemotherapy
and radiotherapy.
The fundamental
goal
of
therapy for
rhabdomyosarcoma (as it is for other solid tumours) is
local region control, and prevention or treatment of
systemic metastasis. Therefore, all patients are treated
systemically with chemotherapy,
locally and
regionally with radiotherapy, surgery or both. Rarely
do occult lymphnodes metastasis occur; hence
prophylactic neck dissection is not warranted. It is not
always possible to do surgical resection of these
tumours, especially where there is intracranial
extension or difficult to reach anatomical areas. Like
in our patient, extensive surgical resection was done
leaving a small tumour in the orbital apex which was
later cleared with chemoradiotherapy.
From the original intergroup rhabdomyosarcoma
study (IRS), Authors recommended multiagent
chemotherapy along with radiotherapy as the mainstay
of treatment and that surgery should be performed