基本HTML版本



International Journal of Clinical Case Reports 2014, Vol. 4, No. 2, 1-5
http://ijccr.biopublisher.ca
2
1 Case
A 7 year old boy was referred to our clinic with a
history of bad breath, nasal obstruction and recurrent
epistaxis from the left nostril for 3 months. The
epistaxis was frank in nature and stained with mucus.
There wasn’t any other bleeding body part. The nasal
obstruction started in the left nasal cavity
progressively increased to involve the right as well. It
was not associated with epiphora or any otologic
symptoms. No headache or loss of consciousness was
reported. He had neither odynophagia nor dysphagia.
On examination he had no lymphadenopathy, had mild
left proptosis with normal eye vision and movements,
reddish left nasal mass with a smooth surface. Other
systems were essentially normal.
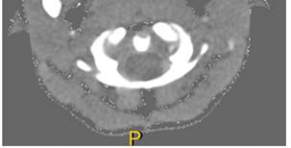
Base line Paranasal CT scan showed slightly
enhancing soft tissue mass 72×77 mm in the nasal
cavity that deviated the nasal septum to the right,
extending to the nasopharynx posteriorly and to the
maxillary and ethmoidal sinuses as seen in Figure 1~3.
In addition there was an 11×16 mm extension of the
mass into the orbit.
Figure 1 Tumour in the left nasal cavity extending to the
nasopharynx posteriorly and to the left maxillary sinus
Biopsy was taken and histology showed embryonal
rhabdomyosarcoma as shown in Figures 4.
Under H and E shows poorly differentiated oval dark
staining cells in a myxomatous stroma with
hyperchromatic nuclei and eosinophilic cytoplasmic
characteristics of rhabdomyoblast with little orientation.
There are few areas of small interstitial collagen
characteristic of Embryonal Rhabdomyosarcoma.
A week later he was taken to theatre where extensive
debulking of the tumour was done leaving a small
residual of tumour in the orbital apex. He was graded
as group III (incomplete resection with gross residual
tumour) according to intergroup rhabdomyosarcoma
study (IRS) standards. He commenced chemotherapy
as per IRS IV protocol, being stage 1 (group III, No,
with no Metastasis) he was given vincristine 1.3
mg/day,
dactinomycin 360 mg/day and
cyclophosphamide 460 mg/day at weekly intervals in
a total of 6 cycles. He handled the chemotherapy very
well.
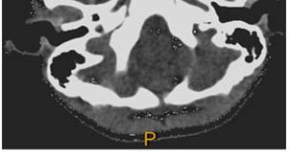
Figure 2 Tumour extending to the left orbit
Figure 3 Tumour in the left orbital apex
Repeated CT scan of the paranasal sinus a month after
completion of the chemotherapy showed over 90%
tumour reduction, with only residual tumour in the
posterior nasal cavity measuring 29×14 mm and no
tumour in the left orbit as seen in Figure 5 and Figure
6. He then received a total of 50 Grays of
radiotherapy.