International Journal of Clinical Case Reports 2015, Vol.5, No. 48, 1-2
2
in 8%. Conventional radiotherapy was used in
8.5% in complement to partial surgical resection.
Patients with a predominant cystic portion underwent
an aspiration of the fluid with instillation of sclerosing
substances in six patients (Yttrium in five patients and
Bleomycine in one patient). Evolution was
characterized by tumour shrinkage in 50%, tumour
stabilization in 33% and tumour progression in 17%.
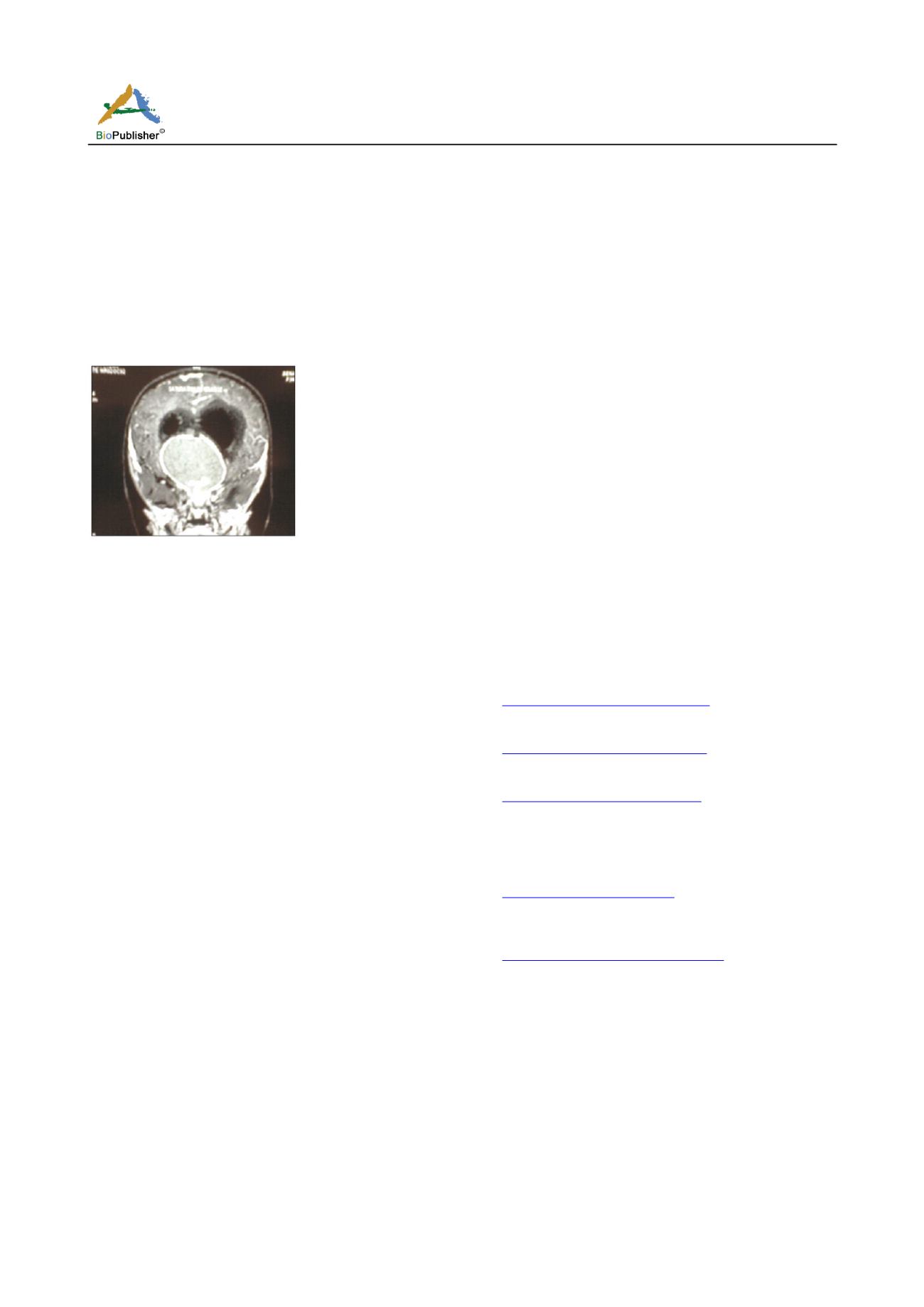
Figure 1
Discussion
Craniopharyngioma represent 5-10% of all childhood
intracranial tumors (Liubinas., 2011). They derived
either from the remnants of the incompletely waned
Rathke’s pouch or a metaplasia of the residual
squamous epithelial rests (Rushing., 2007).
There are two subtypes of craniopharyngioma, the
adamantinomatous subtype which predominates in
children and derive from neoplastic transformation of
epithelial remnants of the craniopharyngeal duct and
the papillary subtype, which predominates in adults
and result from metaplasia of adenohypophyseal cells.
Adamantinomatous craniopharyngioma is characterized by
keratinized squamous epithelium with calcifications
and cystic degeneration. Papillary subtype is
characterized by stratified squamous epithelium
usually without calcifications or cystic degeneration
(Pettorini., 2010). 30-50% of craniopharyngioma
manifest during childhood and adolescence. Initial
symptoms of craniopharyngioma often occur many
years before diagnosis is made. The difficult y to
recognize decreased visual acuity in children may
account for the frequency of visual impairment in our
patients and as reported by others (Müller., 2011).
Craniopharyngioma frequently involve impairment of
the hypothalamic pituitary axis with anterior pituitary
deficits and/or diabetes insipidus (Müller., 2010). The
association of solid, cystic and calcified tumors
components is an important radiological clue to
diagnosis of craniopharyngioma.
The close proximity of craniopharyngioma to vital
structures makes their complete resection very
challenging to the neurosurgeons with a risk of
complications following surgery. Partial resection
followed by radiotherapy seems more favorable
(Müller., 2010).
Recurrences are frequent in pediatric craniopharyngioma
as we observed in our series. Treatment options for
recurrence include repeat surgery, radiotherapy or
instillation of sclerosing agents for predominantly
cystic tumors.
Reference
s
Liubinas S.V., Munshey A.S., and Kaye A.H., 2011, Management of
recurrent craniopharyngioma, J. Clin. Neurosci., 18(4): 451-457
Müller H.L., 2011, Diagnostics treatment and follow-up in craniopharyngioma,
Front Endocrinol (Lausanne), 2: 70
Müller H.L., 2010, Childhood craniopharyngiom a current concepts in
diagnosis, therapy and follow-up, Nat. Rev. Endocrinol., 6: 609-618
Müller H.L., Ebhardt U., Schröder S., Pohl F., Kortmann RD., Faldum A., et
al., 2010, Analyses of treatment variables for patients with childhood
craniopharyngioma results of the multicenter prospective study trial
KRANIOPHARYNGEOM 2000 after three years of follow up, Horm.
Res. Paediatr., 73: 175-180
Pettorini B.L., Frassanito P., Caldarelli M., Tamburrini G., Massimi L., and
Di Rocco C., 2010, Molecular pathogenesis of craniopharyngioma: switching
from a surgical approach to a biological one, Neurosurg Focus, 28: E1
Rushing E., Giangaspero F., Paulus W., et al., Craniopharyngioma, In: Louis
D., Ohgaki H., Wiestler O., Cavenee WK., editors, 2007, WHO
classification of tumours of the central nervous system Geneva: WHO
Press, pp.238-40


