International Journal of Clinical Case Reports 2017, Vol.7, No.11, 45-48
46
human deficiency virus was negative. The tuberculin skin test was positive (diameter at 15 mm). Acid-fast bacilli
test and mycobacterium cultures were negative.
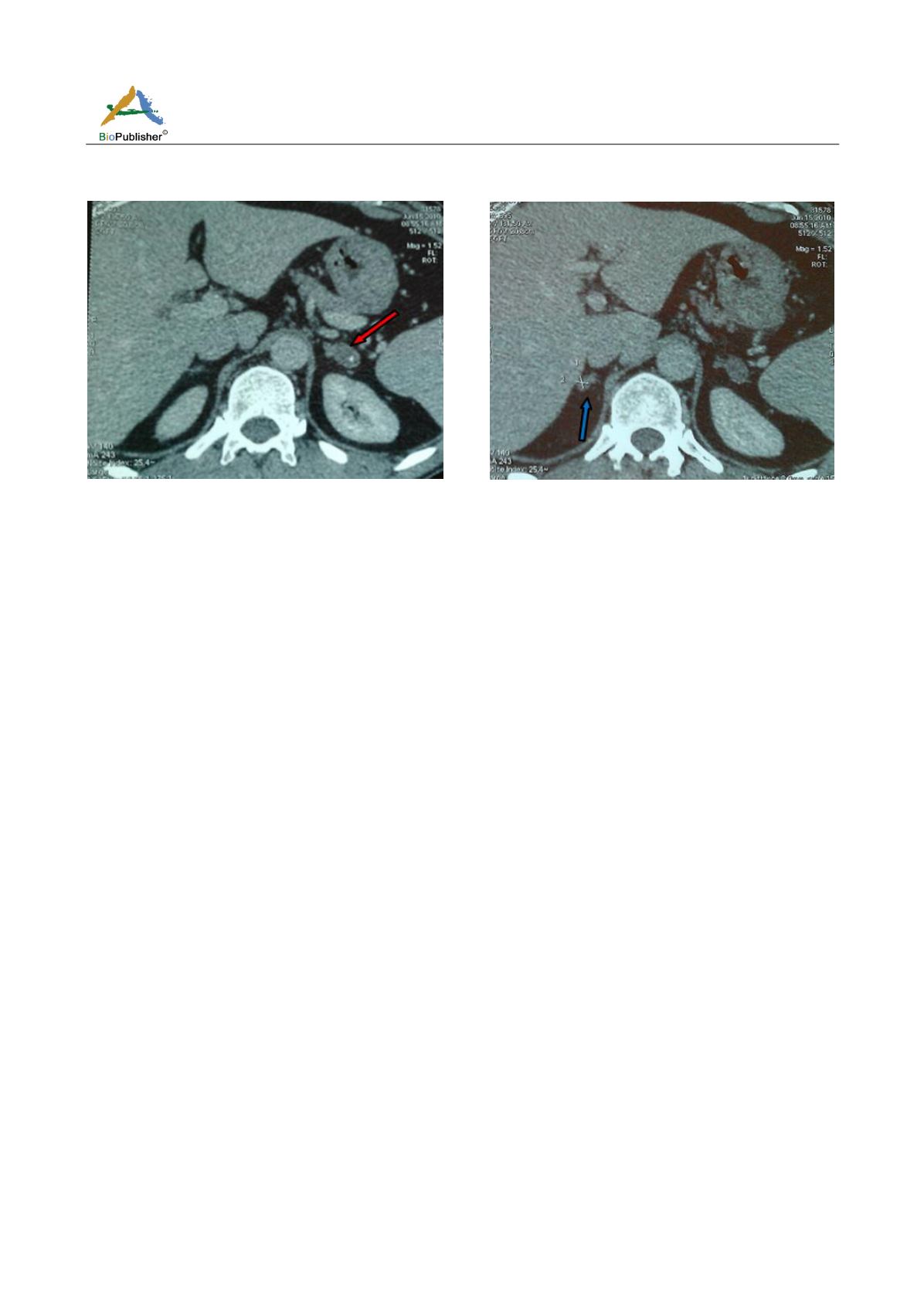
Figure 1 Left adrenal mass with calcification
Figure 2 Right adrenal enlargement
With the background of tuberculosis, adrenal insufficiency diagnosed by laboratory test and positive tuberculin
skin test, bilateral enlargement of adrenal glands was considered most consistent with tuberculosis in our patient.
The patient was put on anti-tuberculosis treatment for six months along with hydrocortisone supplementation. He
was on four-drug anti-tuberculosis therapy (isoniazid, rifampicin, pyrazinamide and ethambutol) for two months,
then on two-drug anti-tuberculosis therapy (isoniazid and rifampicin) for four months.
2 Discussion
Addison’s disease described by Thomas Addison in 1855, when he reported the autopsy findings of six patients
with adrenal tuberculosis is a rare condition with an estimated incidence of 0.8 cases per 100,000 and a prevalence
of 4 to 11 cases per 100,000. Nevertheless, it is associated with significant morbidity and mortality rates if
unrecognized, but once the diagnosis is made; its treatment has spectacular effects (Arlt and Allolio, 2003).
Adrenal tuberculosis was once considered the most common cause of primary adrenal insufficiency. Nowadays,
autoimmune adrenalitis is the most common cause of adrenal insufficiency. However, tuberculosis remains a
common cause particularly in developing country and in immunocompromised persons, it represents 20 to 30% of
cases of Addison’s diseases in some countries (Laway et al., 2013).
Clinical manifestations may take years to become apparent, and asymptomatic infection is not uncommon.
Autopsies studies found 6% cases of adrenal involvement in patients with active tuberculosis (Lamand and Lo,
2001).
Destruction of more than 90% of the adrenal cortex by the infectious process is needed before adrenal failure
appears (Kelestimur, 2004). Both adrenal glands are involved, because Mycobacterium tuberculosis spreads to the
adrenal glands hematogenously at the moment of primoinfection.
Clinical features of adrenal insufficiency relate to the rate of onset and the severity of adrenal deficiency. In many
cases, the disease has an insidious onset and a diagnosis is made only when the patient presents with an acute
crisis during an intercurrent illness. Acute adrenal insufficiency is a medical emergency manifesting as
hypotension and acute circulatory failure and may sometimes lead to the death of the patient (Arlt and Allolio,
2003).
On the other hand, the patient may present with features of chronic adrenal insufficiency such as weakness,
tiredness, weight loss, nausea, intermittent vomiting, abdominal pain, diarrhea or constipation, general malaise,
muscle cramps, arthralgia, and postural hypotension (Arlt and Allolio, 2003).


