International Journal of Clinical Case Reports 2015, Vol.5, No. 44, 1-3
2
Figure 1 Thoracic computed tomography: bilateral ground
glasses at bases
Figure 2 Abdominal computed tomography: spleen enlargement
and a 3-centimeter hypervascularized lower pole renal mass
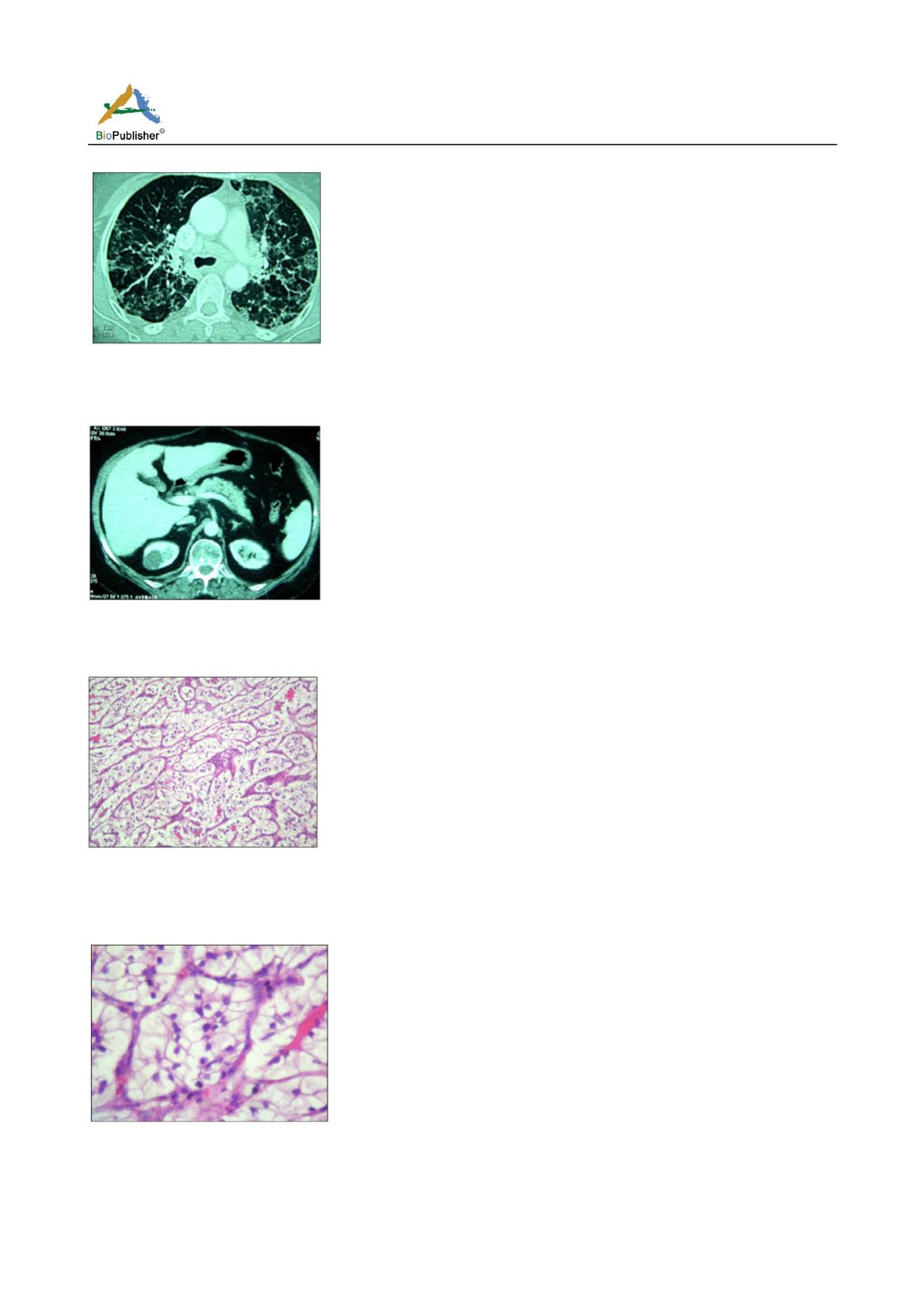
Figure 3 Carcinoma composed of sheets and alveolar structures,
separated by an abundance of thin-walled blood vessels
(HEx10) ?(show with arrow)
Figure 4 Tumor cells with distinct cell membranes and clear
cytoplasm. Nuclei are round and uniform; nucleoli are absent
(HEx40)?(show with arrow)
cases, the diagnosis of systemic sarcoidosis was made
concurrently with the discovery of the neoplasm. We
report hereby the case of a 62-year old patient
admitted for an investigation of chronic dry cough.
She did not complain of any history of lumbar pain
and did not report any urological symptoms. Our
investigations concluded to a sarcoidosis, confirmed
histologically on mediastinal lymph node biopsy and
salivary gland biopsy. CT scan revealed a suspicious
inferior polar mass of the left kidney leading to a
tumorectomy, which confirms the diagnosis of renal
clear cell carcinoma. This means that in our case,
sarcoidosis could be considered as a paraneoplastic
syndrome. Paraneoplastic sarcoidosis is defined as the
onset of sarcoidosis that is coincidental within 1 year
with the discovery of an unsuspected cancer, and is
more commonly reported in hematologic malignancy
(Karakantza et al., 1996). Paraneoplastic sarcoidosis
occurs less frequently in oncologic patients with solid
tumors. To our knowledge, sarcoidosis was diagnosed
concurrently with the detection of malignancy in
patients with kidney cancer as renal cell carcinoma in
two cases (Logan and Bensadoun, 2005; Willis et al.,
2011). These two reported cases consisted of an
undiagnosed condition of sarcoidosis complicating the
staging of renal cell carcinoma. In the two cases, the
patients did not report any symptoms and had no
physical signs related to sarcoidosis, in contrast to our
case, where the patient complained of dry cough and
shortness of breath. This was probably due to a
relatively advanced stage of the sarcoidosis contrasting
with an early stage of the carcinoma. There is a
postulated association between sarcoidosis and
malignancy secondary to an induced T-cell-mediated
host response to soluble antigenic tumor factors
(Brincker, 1986). The antigenic factors may be either
shed by the tumor cells or released during tumor
necrosis. Subsequently, lymphatic vessels transport
the factors to draining lymph nodes where the host’s
immune response, similar to a hypersensitivity reaction,
results in the formation of the non caseating
epithelioid granulomas (Bassler and Birke, 1988). In
our case, pathology of the renal mass demonstrated a
stage T1a clear cell carcinoma. Pathologic margins
were negative. This is to say that although the
diagnosis of malignancy was hazardous, it is considered at
early stage. In fact, the presence of sarcoid reaction
has been shown to have positive prognostic significance


